Suppose I’m right about mental illness. Telling people they’re “sick” might still be a noble lie that makes them feel better. But the reverse is also true: Even if I’m wrong, telling people they’re “sick” might be harmful. Perhaps the mentally ill are better-off believing they can free will their way out of their troubles. As the noble Jason Brennan often reminds us, we should scrupulously separate specific empirical questions from our general philosophical outlook.
In “Effects of a Chemical Imbalance Causal Explanation on Individuals’ Perceptions of Their Depressive Symptoms,” (Behavioral Research and Therapy, 2014), Kemp, Lickel, and Deacon run a fascinating on-point experiment. How does belief in the “chemical imbalance” theory of depression actually affect depression? The set-up: Researchers started with a sample of students who had experienced depression, then:
Participants were randomly assigned to the chemical imbalance condition or the control condition. Following informed consent and collection of demographic information, participants were administered the “Rapid Depression Test” (RDT). The RDT was described as a test of neurotransmitter levels whose results would allow participants to determine whether or not their depressive episode(s) were caused by a chemical imbalance in the brain. Participants were led to believe the purpose of the study was to improve understanding of how individuals respond to learning the cause of their depression, before release of the RDT into clinical practice. The test procedure entailed swabbing the inside of the participant’s cheek with a sterile cotton swab and placing the cotton swab into a sterile collection container. Next, the experimenter (a male undergraduate research assistant wearing a lab coat) instructed participants that he was leaving the experiment room to take their saliva sample to the lab and run the test. The experimenter returned 10 min later with the condition-specific results of the RDT. In the chemical imbalance condition, participants were informed that test results indicated their current or past depression to be caused by an imbalance in the neurotransmitter serotonin. Participants were presented with a bar graph of their test results (see Fig. 1) depicting very low serotonin levels relative to levels of other neurotransmitters, all of which were in the normal range. In the control condition, participants were told their past/current depression was not the result of a chemical imbalance, based on purported test results (and a corresponding bar graph) indicating that all neurotransmitter levels were in the normative range.
Qualitative version of the experimental results:
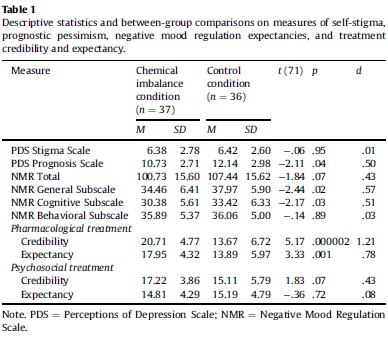
[C]hemical imbalance test feedback increased prognostic pessimism, lowered negative mood regulation expectancies, and led participants to view pharmacotherapy as more credible and effective than psychotherapy. These effects were not offset by reduced stigma, as chemical imbalance feedback had no effect on self-blame. Overall, the present findings suggest that providing individuals with a chemical imbalance causal explanation for their depressive symptoms does not reduce stigma and activates a host of negative beliefs with the potential to worsen the course of depression and attenuate response to treatment, particularly psychotherapy.
To repeat, none of this shows the chemical imbalances view is false. But it does show that accusing Szaszian skeptics of lack of empathy for human suffering is unfair. Telling troubled people, “Your bad brain chemistry is beyond your control, it’s not your fault” may sound compassionate, but they seem to hear a bleaker message.
READER COMMENTS
Kevin Erdmann
Feb 14 2016 at 11:03pm
[Comment removed. Please consult our comment policies and check your email for explanation.–Econlib Ed.]
Richard
Feb 14 2016 at 11:51pm
Yes, the belief in free will is strong, and is the basis of most religions. It lasts because it is an evolutionary adaptation. In every work environment I’ve been in, the good ones were the ones who believed that they got what they deserved while the lazy ones blamed everything on forces beyond their control.
It’s true that everything is really about chemicals and biology. But it’s just as true that humans respond to things like incentives and ideas.
HM
Feb 15 2016 at 1:44am
[Comment removed. Please consult our comment policies and check your email for explanation.–Econlib Ed.]
Seb Nickel
Feb 15 2016 at 8:49am
What reason is there to think that it’s harder to “free will your way” out of a chemical imbalance than out of any otherwise-accounted-for depression?
It makes sense that telling people they have a chemical imbalance is harmful to them IF they believe this, and I understand many people do believe it. But do they believe it for good reasons?
John Alcorn
Feb 15 2016 at 10:42am
Bryan,
Elsewhere in this fascinating article, the authors state:
Thus there seems to be an important distinction between (a) informing a subject that her depressive symptoms are caused by chemical imbalance and (b) informing her also, emphatically, that the chemical imbalance is malleable.
A related question is: What techniques might malleate biology (chemical imbalance) in healthy ways? Pharmacotherapy is a direct technique, but there are also indirect techniques (e.g., regular physical exercise).
Another related question is: Is it necessary for the subject to believe that pharmacotherapy (or an indirect technique) is effective, in order for pharmacotherapy to be effective?
Still another question is: Is it sufficient for the subject to believe that pharmacotherapy (or an indirect technique) is effective? In this case (sufficiency of belief), a placebo pill could be as effective as pharmacotherapy. By contrast, there is no placebo for regular physical exercise.
Doubtless, psychologists have studied specifically these questions, and other pertinent distinctions. Might you or your informed readers provide pointers to the best articles?
Thank you!
David Condon
Feb 15 2016 at 10:48am
In the paper, you talk about how unusual preferences are not evidence of sickness however it seems you’re really making a claim about people’s underlying intrinsic motivation. If some people have perfectly normal intrinsic motivation, but still display unusual preferences, then this suggests health care might be able to help them better achieve their goals, assuming there is an objective reality. You’re claiming that unusual preferences are due to disparities in their intrinsic motivation. You’re claiming unusual preferences are not due to disparities in perception. You insist on using the term preference throughout the paper (a behavioral term) even though the paper is really about cognitive processes.
The honest answer of why medications are so widespread is that medications are cheap, and easily coordinated. There are some people whose personal negative externality as you put it is so large that it is impossible for them to function in day-to-day life. Taking care of these people is exorbitantly expensive, and medications are generally the cheapest way to handle the problem in many cases.
While some of the time this medication may lead to a change in their intrinsic motivation in a way the patient does not desire, in many other cases it probably reduces errors of perception. Many normal people state a preference for antidepressants or for anxiety medication both before they take them and after. Is it wrong to give it to them? For many of the mentally ill, they may be unable to make long-term plans. While certain changes may be against their immediate motivations, they are in alignment with their motivations that they will have in the majority of the rest of their life even if no change is made. If the individual is unable to perceive these later events, is it wrong to make a choice for them to help them later in life?
As for your evidence here, given the sample size, I’d say all you’ve demonstrated is that immediately after hearing the results of a pharmacological test of depression, the participant has a much more positive view of pharmacological treatment. There is no evidence of attenuation of the effectiveness of psychotherapy as the authors claim.
Tom West
Feb 15 2016 at 11:44am
I fail to see how this finding would not be identical when applied to other illnesses like cancer, diseases, etc.
Telling someone that there is a diagnosis for the symptoms almost certainly inclines them towards pharmacological solutions.
Perhaps we should be insisting that people use free-will to defeat those illnesses, along with the obvious corollary that if they are succumbing to those diseases, that is a failure of desire to be well.
Peter Gerdes
Feb 15 2016 at 11:51am
[Comments removed pending confirmation of email address. We have attempted to contact you many times previously. This is your final notice. If you want your comments published on EconLog, please email the webmaster@econlib.org to discuss your comment privileges. A valid email address is required to post comments on EconLog and EconTalk. We have bent over backwards for you. Email us from a valid email address if you would like your comment privileges restored.–Econlib Ed.]
Chris Wegener
Feb 15 2016 at 12:48pm
I have, with amusement, followed your description of mental illness as a choice for sub optimal intrinsic motivations.
Your points are very much the flip side of a conversation with a seriously mentally ill person. That person cannot be convinced that they are not “normal” in so far as normal is defined by an ability to navigate reality in some manner to not leave them conversing or reacting to delusion or even hallucinations. It is impossible to motivate a clinically depressed person “to just snap out of it.” It is impossible to convince a paranoid individual that there are not sinister conspiracies to kill them.
Just as you, a “normal” person cannot understand the difficulties that a mentally ill person faces in their attempts to function.
To demonstrate what I mean, I would suggest that for a week you assume the intrinsic motivations of a homosexual. Act and believe that you are attracted to members of your gender. See yourself repulsed by the thoughts of attractions to the opposite sex.
Let’s talk after you have tried to change your “intrinsic motivations.”
Mark Bahner
Feb 15 2016 at 12:52pm
We could make that supposition, but it’s almost certain that you’re wrong. According to the bureau of labor statistics, there are more than 25,000 psychiatrists in the U.S., and on average they make more than $180,000 per year. What are the odds that they’re all wrong (and therefore the people paying them those wages are also wrong), and an economist (who I assume has never taken a single course even closely related to psychiatry) is right?
Well, let’s look at an analogous situation. Perhaps gay people are better off believing they can pray their way to heterosexuality. The main problem with that belief is that the evidence is overwhelming that they won’t be able to do so.
Or let’s look at perhaps an even better analogy…was Alan Pean better off because the staff in St. Joseph Medical Center in Houston apparently (and amazingly) didn’t realize he was mentally ill? No, he was almost certainly worse off.
Would he be better off in his life if he never took geodon (an anti-psychotic medication) and simply tried to “free will” his way out of psychotic episodes? That’s not a rhetorical question. Do you think he would be better off not taking any anti-psychotic medication during psychotic episodes?
Philo
Feb 15 2016 at 6:39pm
Increased prognostic pessimism? Why? If I believed that my depression was caused by a chemical imbalance, I would move heaven and earth to find a substance I could ingest that would correct the imbalance (or, as John Alcorn remarks, to find an indirect way of affecting my body chemistry). I would expect that there is such a substance (or such an indirect treatment), and so I would be optimistic about my prognosis, as compared with my attitude if I had no idea what was causing my depression. And I would blame myself only if I did not try very hard to find the appropriate treatment–again compared to the situation where I did not know the cause, and therefore thought there was some probability that I was, indeed, to *blame*.
In short, the study’s findings seem unreasonable.
AlexR
Feb 16 2016 at 12:43am
How are “troubled people” hearing “a bleaker message”? I don’t see much in the study inconsistent with rational, optimizing behavior. Being “troubled” is not so different from being “hungry.” In both cases, the consumer seeks to alleviate the condition.
Suppose someone considered to be credible tells a hungry person that, as between two bowls of food on the table, the one containing vegetable lomein is not as filling as the beef lasagna. The hungry person might take the information to heart, desire the lasagna and think negative thoughts about Chinese food “leaving you hungry an hour later.”
Likewise, a troubled person told that addressing a chemical imbalance is the way to go may well seek drug therapy and think negative thoughts about behavior modification therapy.
The only potentially irrational aspect to the story is subjects naively taking psychologists at their word, when their double-blind experimental design necessitates systematic lying.
Sasz was right, of course, in his critique of involuntary psychiatric hospitalizations. But his claim that mental illness is a “myth” is as silly as a claim that hunger is psychosomatic. The customer is always right.
Colombo
Feb 16 2016 at 1:05pm
That was a good defense, Bryan.
It surprises me to see how many people who call themselves libertarians are not also metaphysical libertarians. I guess this is also as inconsistent as the fact that most of the philosophers who are metaphysical libertarians are not libertarian in any other sense. And it is funny that these two groups don’t cancel out mutually.
It is in the best interests of all politicians that people believe that mental illness is a thing. If the “chemical imbalance theory” was harmful to our democratic tyrants then it would have never been formulated, and it would be removed from the books, and from the recorded history.
Scientists are helpless. They beleive they can outsmart politicians. They can’t, and they have been abused by them. People who “believe” in Science don’t realize how weak their heroes are to political manipulation.
Nathan W
Feb 17 2016 at 7:19am
I think “sick” is entirely the wrong word. This might be conducive to an understanding of being sick and getting better. It would be better to have terminology which reflects whether one is referring to a short term issue or an issue which is likely to be permanent.
Various chemical imbalances or non-ideal brain chemistry is real. But absolving people of personal responsibility, or alternatively inferring that their own mental endeavours to maximize their mental, is not good.
I think part of the trouble here is that most of mental health is basically pseudo-science, generally based on self-reported symptoms, almost never based on any sort of genuinely empirical thing such as brain chemistry (you happen to refer to an exception in this post, however, wrt seratonin and depression).
Also, “chemical imbalance” might imply that things are GENERALLY awry in their brain. The term does a disservice to understanding what is actually going on. Is it really so wordy to just say “high/low seratonin”?
Imagine receiving the news “you have a chemical imbalance in your brain” (sounds pretty defective) to receiving the news “you have low seratonin levels and this is associated with depression, which you have been complaining of” (sounds like a pretty specific and straightforward issue which can be addressed).
For practical purposes, I suggest a clinician could optimally say the following sort of thing in the situation referred to above: “your seratonin levels are low, and we can treat this using medication, but there are plenty of physical and mental exercises that will [the certainty of “will help” promotes a lot of agency] also help, and here is how you can explore these if you wish”.
Nathan W
Feb 17 2016 at 7:24am
The “God will fix your chemical imbalance” is probably the worst possible thing. I’m half inclined to wonder whether it should be criminal for certain kinds of professionals to dispense such advice, perhaps even including spiritual leaders.
This is very different from saying something like “God will certainly be looking out for you” without suggesting that God will fix everything. Actual chemical treatment plus a belief that God is doing his/her best is probably useful. But, even then, this takes away agency. The patient is putting it all on God, which absolves them of doing any hard work themselves, such as getting into an exercise routine, eating right, getting out more even if they don’t really want to, or performing various types of mental exercises.
Nathan W
Feb 17 2016 at 8:01am
Seb – “What reason is there to think that it’s harder to “free will your way” out of a chemical imbalance than out of any otherwise-accounted-for depression?”
Because in the first case, the cause is the “chemical imbalance”. I would put good money down that no amount of free will could have much more than a marginal effect on that imbalance. Other depressions may be caused by things such as a divorce, job loss, etc., which is a rather different situation.
John – “Is it necessary for the subject to believe that pharmacotherapy (or an indirect technique) is effective, in order for pharmacotherapy to be effective?”
Very interesting question. I suggest that if the patient does not believe it will work, the “chemical imbalance” itself could be treated while the patient may be so stuck in certain thinking patterns, behaviours, etc., for them to fail to get out of the depression.
Tom – “I fail to see how this finding would not be identical when applied to other illnesses like cancer, diseases, etc.”
Because your head has more control over your head than your liver. Your head cannot stop liver cancer (99.9999% sure) but using free will and an activist plan to reform certain behaviours or thinking patterns may be at least partially effective, even in failing to treat the underlying “imbalance”.
Mark – “What are the odds that they’re all wrong … and an economist … is right?”
A lot of practicing psychiatrists were trained before there was much of any knowledge whatsoever about anything about the brain, from a science-based neurology perspective. I wouldn’t be surprised if a pretty free thinking, intelligent and broadly informed economist might beat the average after having taken some time to inform themselves.
It’s hard to teach an old dog new tricks. And people who are stuck in their ways with old fashioned beliefs are notoriously difficult to bring around to knew knowledge. Both of which cliche situations are conducive to a complete newcomer to the field having more sensible things to say than the average current practitioner. For starters, Bryan could not possibly be suffering from over-confidence in a situation of stale/false old knowledge.
“Well, let’s look at an analogous situation. Perhaps gay people are better off believing they can pray their way to heterosexuality.”
There’s a really big difference between something with a genetic cause and something where, for whatever reason, the brain has gotten into some new normal which is low seratonin.
“Do you think he would be better off not taking any anti-psychotic medication during psychotic episodes?”
Bryan is speaking of low seratonin. The brain chemistry is well understood. I think comparing this to mental illnesses which benefit from essentially zero understanding of the brain malfunctions involved is not quite on the mark. For example, it is known that regular exercise can help with seratonin levels, whereas there is no analogous knowledge with respect to “psychotic episodes” (a blanket term which is broadly inclusive of all sorts of things which are basically unreltaed).
Mark Bahner
Feb 17 2016 at 12:16pm
And when did Bryan get his training about the brain? (That’s essentially a rhetorical question. I will bet you $50 that Bryan has never passed any university-level course on the brain.)
This sort of attitude really bothers me…the idea that some amateur who, as far as I can tell, hasn’t even spent much time on the subject, can tell 25,000 well-paid professionals, who have cumulatively spent literally billions of hours studying something, that they don’t have the slightest idea what they’re talking about.***
***P.S. Of course, some people might think a similar situation is occurring when I criticize the economics profession for not recognizing the spectacular economic growth that will likely occur as a result of artificial intelligence (world per-capita GDP growth rates above 10 percent per year within the next 10-30 years). But that’s of course different…because I’m right. 🙂 And Bryan is clearly wrong about mental illnesses simply representing “extreme preferences.”
Jameson
Feb 17 2016 at 12:59pm
Love this.
Mark Bahner
Feb 17 2016 at 6:10pm
You love specious sloganeering? Bryan is saying that even if he’s wrong (which he almost certainly is) it would be better for the people suffering from mental illness if everyone behaved as though Bryan was right. That’s obviously nonsense, and it doesn’t reflect well on Bryan that he doesn’t admit it.
Bryan is essentially saying that people who are clinically depressed–who have the recognized psychiatric illness of depression–should be told that their depression is merely some bizarre “extreme preference.” That’s appallingly wrong, and it would probably do great harm to people with depression if people followed Bryan’s advice. (Which thankfully they almost certainly won’t.)
Comments are closed.